-
The disease in numbers
The damaged process happens through the excessive deposition of collagen and other connective tissue proteins, which cause progressive scarring of lung tissue through inflammation and fibrosis. This disorganized tissue remodeling impairs the vital role of the lungs in respiration with devastating consequences in terms of functional capacity, quality of life and increased mortality.1The prevalence of ILD has been estimated as 81/100,000 in males and 67/100,000 in females.2
Within ILD, the most common classification is Idiopathic Pulmonary Fibrosis (IPF). In Europe, IPF prevalence ranged from 1.25 to 23.4 cases per 100,000 population.3
Furthermore, ILD occurs in 15% of patients with connective tissue disease (CTD), which is a group of autoimmune diseases from which the most common, rheumatoid arthritis (RA), affects between 0.5% to 2% of the general population in the USA.4
![]()
Watch our educational video
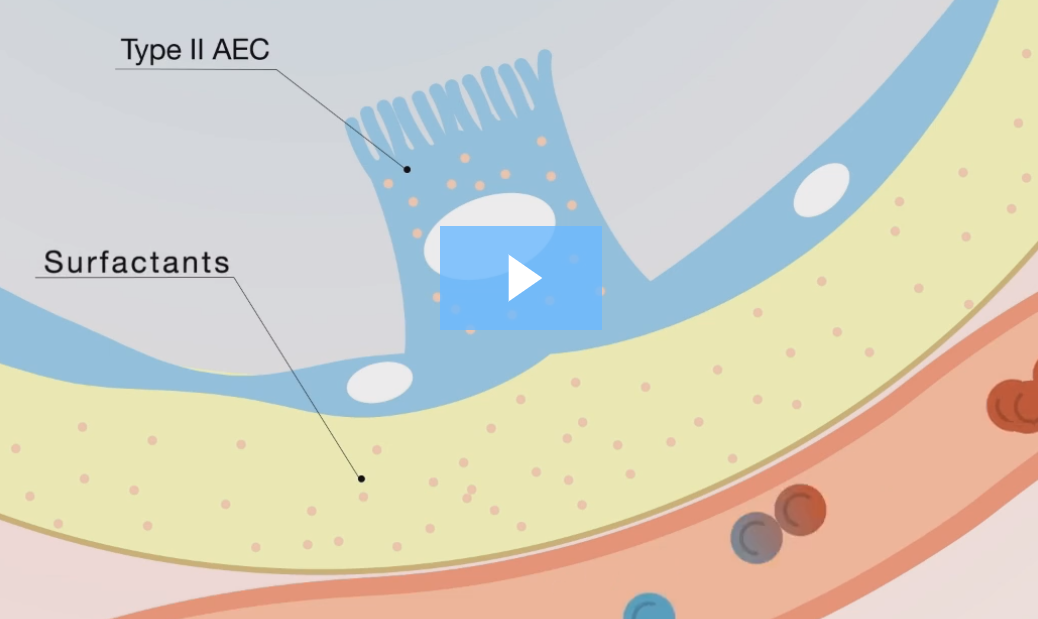

Interstitial Lung Disease (ILD)
Millions of people suffer from lung diseases that affect any part of the respiratory system including the airways, the air sacs (alveoli), the interstitium, the blood vessels, and the pleura.
A large and heterogeneous group of diseases called Interstitial Lung Disease (ILD) affect the interstitium, a thin layer of cells between the alveoli, which contains blood vessels and cells that help support the alveoli, allowing efficient gas exchange.
